
Hormones are chemical messengers that help regulate many functions in the body, including growth, metabolism, reproduction, stress response, and the hair growth cycle. When hormone levels are balanced, they support normal follicle activity. When they shift or become abnormal, they may contribute to shedding, thinning, miniaturization, or changes in hair texture.
Hormonal hair loss can affect both men and women, but it does not always mean a hair transplant is needed. Thyroid imbalance, postpartum shedding, menopause, PCOS, androgen sensitivity, stress hormones, and nutritional factors can all influence the hair cycle. Before choosing treatment, the cause should be understood. If hair loss becomes stable, genetic, and advanced, patients may later consider hair transplant options in Turkey after a doctor-led evaluation.
A hormone is a chemical messenger produced by endocrine glands. Hormones travel through the bloodstream and communicate with specific cells or organs. They help regulate many physiological functions, including metabolism, growth, fertility, mood, skin health, and hair follicle behavior.
Hormones can be grouped in different ways, but two common categories are:
Because hair follicles are biologically active structures, they can respond to hormonal changes. This is why androgen imbalance, thyroid disease, pregnancy, menopause, and stress-related hormone changes can all affect hair growth.
A hair follicle is a small structure in the skin where hair growth begins. Each follicle contains living cells, blood supply, sebaceous glands, and signaling structures that help control hair growth, rest, shedding, and regeneration.
The follicle is responsible for producing the hair shaft, supporting pigmentation, receiving nutrients, and cycling through growth and shedding phases. When hormones affect the follicle, the result may be thicker hair, shedding, miniaturization, or reduced hair quality depending on the hormone and the patient’s sensitivity.

The hair follicle is made of several important structures:
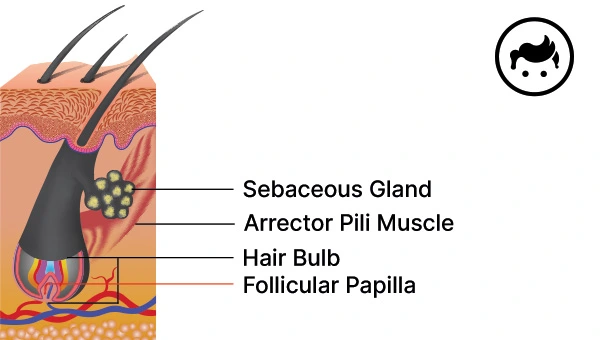
The sebaceous gland releases sebum, which helps lubricate the scalp and hair. Hormones, especially androgens, can influence sebum production. When sebum production is excessive or when inflammation is present, some patients may experience oiliness, flaking, itching, or scalp irritation.
Scalp inflammation does not always cause permanent baldness, but persistent symptoms should be evaluated. You can read more in our guide on seborrheic dermatitis hair loss.
The arrector pili muscle is a small smooth muscle attached to the hair follicle. It contracts during piloerection, commonly known as goosebumps. Although it is not the main cause of hormonal hair loss, it is part of the follicle’s supporting structure.
The bulge area contains cells involved in follicle maintenance and regeneration. Damage to important follicular structures can affect the hair cycle and may contribute to poor hair quality or hair loss in some conditions.
Supportive treatments such as stem cell treatment are often discussed in relation to follicle regeneration, but they should not be presented as a guaranteed cure for baldness. Suitability depends on diagnosis and medical evaluation.
The hair bulb is the lower part of the follicle where active cell division helps produce the hair shaft. It also contains melanocytes, which influence hair color. The bulb depends on blood supply, nutrients, and biological signaling for normal hair production.
The follicular papilla, also called the dermal papilla, helps regulate hair growth signals. Its size and activity can influence hair shaft thickness. Hormones and growth factors can affect signaling in this region, which is why hormonal changes may influence hair density and growth quality.
Several hormones can affect hair follicles. The most important are androgens, estrogens, progesterone, thyroid hormones, and stress-related hormones.
Testosterone is a steroid hormone produced mainly in the testicles in men and in smaller amounts by the ovaries and adrenal glands in women. It plays a role in reproductive health, muscle mass, bone health, libido, and body hair development.
Testosterone itself is not always the direct problem in scalp hair loss. The key issue in male pattern baldness is often how genetically susceptible follicles respond to DHT, which is formed from testosterone by the enzyme 5-alpha reductase.
DHT is one of the most important hormones in androgenetic alopecia. In genetically susceptible scalp follicles, DHT can bind to androgen receptors and contribute to follicle miniaturization. Over time, the follicle produces thinner, shorter, weaker hairs until visible thinning appears.
In men, this often appears as temple recession, frontal thinning, or crown thinning. The Norwood Scale is commonly used to describe the progression of male pattern hair loss.
In women, androgen-related thinning may appear as diffuse thinning across the top of the scalp, widening part line, or reduced density. For more detail, review our guide on female pattern baldness.
Estrogen can help support the anagen, or growth phase, of the hair cycle. This is one reason some women notice thicker-feeling hair during pregnancy when estrogen levels are higher.
After childbirth, estrogen levels fall, and many hairs can enter the shedding phase at the same time. This can lead to postpartum shedding, which is often temporary. Menopause-related estrogen changes may also contribute to changes in hair density and texture.
If shedding is severe, persistent, or combined with fatigue, menstrual changes, acne, weight changes, or other symptoms, medical evaluation is recommended.
Progesterone is involved in menstruation and pregnancy and interacts with estrogen and androgen pathways. Its relationship with hair growth is indirect and can vary between patients.
Low or shifting progesterone levels may be part of a broader hormonal picture, especially around pregnancy, postpartum changes, perimenopause, or menopause. However, hair loss should not be attributed to progesterone alone without proper evaluation.
Thyroid hormones help regulate metabolism and influence the hair growth cycle. Both hypothyroidism and hyperthyroidism can contribute to diffuse shedding, brittle hair, dryness, or reduced density.
Thyroid-related hair loss may improve when thyroid levels are managed, but regrowth can take time. If hair loss is accompanied by fatigue, weight change, cold or heat intolerance, mood changes, or menstrual irregularity, thyroid testing may be considered by a doctor.
DHEAS is an adrenal hormone that can act as a precursor to androgens and estrogens. Abnormal adrenal hormone patterns may be relevant in certain endocrine conditions, but DHEAS should not be interpreted in isolation.
If a patient has symptoms such as acne, excess facial/body hair, irregular periods, rapid shedding, or signs of androgen excess, a medical professional may evaluate adrenal and ovarian hormone markers together.
Hormones can affect hair follicles by changing the length of the growth phase, increasing shedding, altering oil production, influencing inflammation, or causing follicle miniaturization in genetically susceptible areas.
The effect depends on the hormone, the patient’s genetics, the scalp area, and whether there is an underlying medical condition. For example, DHT may contribute to scalp follicle miniaturization in male pattern baldness, while estrogen changes may contribute to postpartum or menopause-related shedding.
Yes. Hormones are only one part of the picture. Hair loss can also be caused or worsened by genetics, nutrient deficiencies, medications, illness, scalp inflammation, autoimmune disease, stress, aging, and physical or chemical damage.
That is why diagnosis matters. A patient with DHT-related male pattern baldness needs a different plan than a patient with thyroid disease, iron deficiency, postpartum shedding, or seborrheic dermatitis.
For related diagnosis pages, review:
The hair growth cycle has several phases. Hormones can influence how long hair remains in each phase.
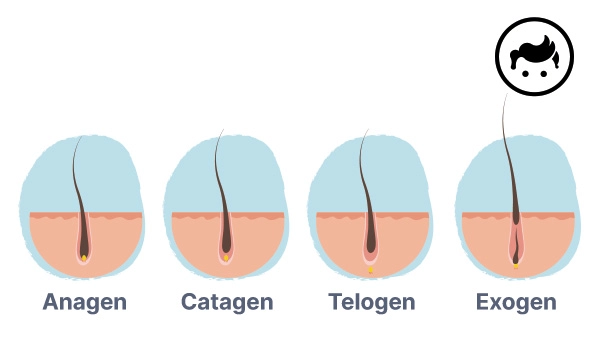
The anagen phase is the active growth stage. Hair grows from the follicle during this phase, and the length of the anagen phase helps determine how long hair can grow. Hormones, genetics, nutrition, age, and health can all influence this phase.
The catagen phase is a short transition stage. Hair growth slows, and the follicle prepares to enter the resting phase. This is a normal part of the cycle.
The telogen phase is the resting stage. When too many hairs enter telogen at once, noticeable shedding can occur. This can happen after stress, illness, childbirth, thyroid imbalance, rapid weight loss, or medication changes.
The exogen phase is when older hairs are released from the scalp. Losing around 50 to 100 hairs per day can be normal, but sudden or excessive shedding should be evaluated if it continues or is associated with other symptoms.
Treatment depends on the cause. Hormonal hair loss should not be treated blindly because the right plan differs for DHT sensitivity, thyroid disease, postpartum shedding, menopause, PCOS, iron deficiency, or stress-related shedding.
For a broader comparison of treatment options, review our hair loss treatments for men guide and our general hair treatments guide.
A hair transplant may be considered when hormonal or genetic hair loss has created a stable, transplantable pattern and the patient has enough safe donor hair. It is not usually the first step for active thyroid disease, postpartum shedding, uncontrolled PCOS-related shedding, active scalp inflammation, or untreated deficiency-related hair loss.
In suitable cases, doctors evaluate the hair loss pattern, donor area, age, medical history, and expectations. The how many grafts do I need guide explains how graft planning begins.
Modern planning may include FUE hair transplant extraction and DHI hair transplant implantation when suitable. If surgery is appropriate, reviewing transparent Turkey hair transplant packages can help you understand graft planning, technique, hotel, transfers, and aftercare together.
Yes. Hormonal changes can contribute to hair loss by disrupting the growth cycle, increasing shedding, changing scalp oil production, or causing follicle miniaturization in genetically susceptible patients. DHT, thyroid hormones, estrogen changes, postpartum shifts, menopause, and PCOS-related androgen imbalance can all affect hair.
DHT, or dihydrotestosterone, is the hormone most closely linked to male pattern baldness. In genetically susceptible follicles, DHT can contribute to miniaturization, causing hair to become thinner and weaker over time.
Falling estrogen levels can contribute to shedding in some women, especially after childbirth or during menopause. However, hair loss is often multifactorial, so thyroid function, iron levels, stress, genetics, and scalp health may also need evaluation.
Yes. Both hypothyroidism and hyperthyroidism can disrupt the hair growth cycle and cause diffuse shedding or brittle hair. Thyroid-related hair loss may improve when thyroid levels are properly managed, but recovery can take time.
Sometimes, but not always. If the hormonal issue is active or temporary, the underlying cause should be treated first. A hair transplant may be considered only when the hair loss pattern is stable, the scalp is healthy, and the patient has enough safe donor hair.





You are just one step away from getting a completely free medical analysis.
Close windowWhich image best describes your current hair loss? Or use Voice Input.
Your age helps us determine the stability of your donor area.
At your age (18-23), hair loss is likely still progressing. We highly recommend preventative medical treatments.
Get Info on TreatmentsHave you ever had a hair transplant before?
Do you have any of the following health conditions?
Calculating graft density and hairline design.
Estimated Graft Need
🏆 Highly Recommended: VIP
We strongly recommend the VIP Package as it includes sedation/anesthesia, ensuring a completely comfortable and painless procedure.
📸 Please prepare these 3 photos for the doctor (Front Area, Top Crown, Back Donor):